Photo by Phenyo Deluxe on Pexels.com
The Problems:
- Teenage endometriosis is much more common than most realize. Therefore, unfortunately, the diagnosis may not even be considered.
- The time between the onset of symptoms and the diagnosis of endometriosis has been demonstrated in various studies to range between 7-10 years, even amidst today’s health care advances. This delay is most unfortunate in teenagers, because it may alter quality of life to such a degree that the ‘flower doesn’t bloom.’
- Even after an accurate diagnosis, definitive treatment is often delayed further for reasons that we will discuss.
We can address these problems proactively and significantly improve our service to those who suffer.
In order to know when health care providers and parents should begin thinking about the possibility of endometriosis, I want to first suggest a few boundaries to the normal path through menarche:
To begin, the age of menarche is extremely variable. It is influenced by heredity, nutrition, emotional stability, and body fat percentage (for starters). I have never noted an excess of early or late menarche in patients who were later diagnosed with endo.
Menarche may be associated with variable amounts of menstrual bleeding and clotting. Menstrual intervals and durations may also vary considerably for 12 to even 36 months. Most of the time, these variables are secondary to the time it takes to develop cycles that are consistently ovulatory. While later in reproductive life, large ovarian endometriomas may alter menstrual cycles; this is not a common problem in teenagers.

Photo by Pixabay on Pexels.com
Dysmenorrhea (menstrual cramping) is also widely variable in ‘normal’ teenagers as they begin to menstruate. Some have few or no complaints, yet others may be temporarily incapacitated. When I am evaluating teenagers, I am most interested in observing the trend in the degree of their dysmenorrhea and other symptoms (see below) over the first several months and even the first two years. I am encouraged when I hear that the ‘menstrual experience’ stabilizes, and becomes a predictable event during which the amounts of bleeding, clotting, and cramping are fairly consistent from one cycle to the next. Further, I am somewhat reassured if after a ‘bad’ period occurs, one that is back to the usual follows it.
Here is the first important observation. When I hear that menstrual events are progressively worsening from month to month and year to year, I want to find an explanation. We will look at a list of things that should be considered (“differential diagnosis”) in the following paragraphs, but the individual with a trend of progressively worsening symptoms needs a diagnosis – and most of the time we can provide it.
Other menstrual symptoms may also occur in ‘normal’ healthy teenagers. These symptoms may include but are not limited to nausea, diarrhea, mood swings, bloating, breast tenderness, and fatigue. Again, in the normal situation, I expect to see that these symptoms are adapted to with a minimal use of medication within the first several months to years. A history of progressively increasing symptoms demands evaluation.
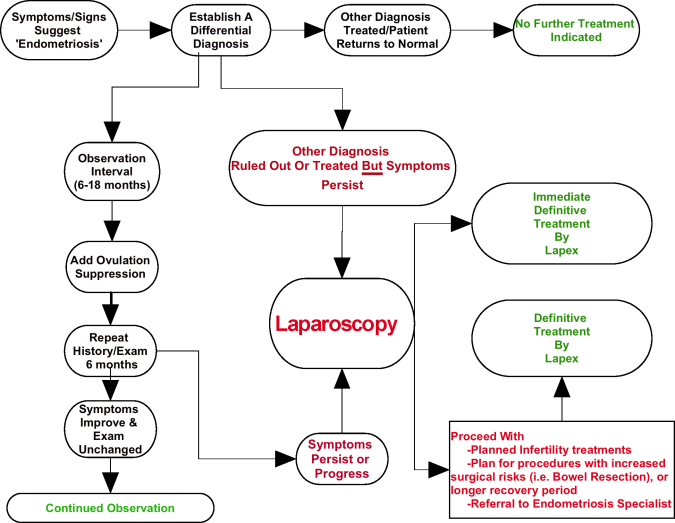
The second important observation is this: some symptoms should be promptly evaluated. These include menstrual bowel movements or diarrhea associated with bleeding, prolonged nausea and vomiting, consistently painful ovulation (mittleschmerz), unilateral ovulation pain, and pelvic pain apart from menses. When a teenager’s passage through menarche falls outside of the above listed boundaries, families and health care professionals should be prepared to apply an appropriate differential diagnosis. This means that through the use of a good history, careful physical exam, special testing procedures and laboratory testing, inappropriate diagnoses are ruled out and no longer considered. Most of the time this can be done in one or two office visits. In teenagers, endometriosis is often a diagnosis of exclusion after all other reasonable possibilities have been ruled out.

Photo by Pixabay on Pexels.com
Below is a list of possible diagnoses that the professional should be prepared to rule in or out. These are not necessarily in any order.
Inadequate education leading to fear:
- Menarche can be frightening when unexpected and misunderstood. Some teenagers are not mentally capable of understanding the reproductive cycle, and rarely others have been so sequestered that they do not expect their first period.
Physical abuse:
- Sadly, in our society today, young people still remain vulnerable to those who impose their will on them. I have evaluated many teenage girls because of their inability to adapt to menses only to become aware that their physical complaints were actually a manifestation of their anxiety and shame relating to their ongoing or past experiences of being abused.
- Healthcare providers must at least consider this possibility as part of their ‘differential diagnosis’.
Other unnamed needs:
- I have evaluated several patients that really only wanted contraception, but were afraid for various reasons to make an appointment primarily for that reason. They simply told those responsible for them that they were having severe menstrual pain.
Drug seeking behavior:
- Another subgroup of teenagers that might express complaints related to menses that are outside the boundaries that I have mentioned above is made up of individuals that want narcotics or other drugs that they have become dependent on.
Imperfectly developed anatomy:
- This includes imperforate hymen, incompletely developed vagina, and abnormally developed uterus.
Pelvic infection:
- In this country, pelvic infection is almost always associated with a sexually transmitted microbe.
- A teenager who has never been sexually active can be considered extremely unlikely to have a pelvic infection unless there has been recent surgery in the abdomen or pelvis or pelvic instrumentation such as associated with the insertion of an IUD (intrauterine contraceptive device).
Unusual pelvic tumors or growths:
- There are several tumors that we may see in teenagers that may or may not be associated with symptoms. Thankfully, most of them are benign. A good example of this would be a teratoma (or Dermoid).
When the above considered explanations for significant menstrual and pelvic complaints have been considered, and a diagnosis is not obvious, ‘endometriosis’ should be the presumptive diagnosis until proven otherwise.

Further Commentary
Examining young patients: the physical examination of frightened, anxious teenagers who are in pain is often a significant challenge. Here are my suggestions.
- My patient decides for herself if she will be examined and if there are any limitations she wants to put on the exam. If she elects to forego any part of the exam, I explain the advantage of doing that part to her and document her decision. Interestingly, by the time the second office visit occurs, and the patient develops a confidence in my desire to help her, and my willingness not to force her into anything, she often acquiesces to an exam.
- Unless she prefers to have only my nurse in the exam room with her, I want her to have an additional person whom she trusts to be there with my nurse and me. My friendly and encouraging nurse is essential to helping me establish a suitable environment for the exam.
- In my exam room patients are covered from top to bottom with gown/drape/blanket/etc. It helps the patient keep her modesty to only uncover one small area at a time and then recover it afterwards. It is particularly important with a teenager to explain every step in your exam process and its purpose.
- If the patient uses tampons for protection during menses, I may suggest a vaginal probe ultrasound in lieu of her first pelvic exam. I allow her to place the probe into the vaginal canal before I try to manipulate it. She can remain entirely covered in this way.

Photo by Pixabay on Pexels.com
Emergency Room experiences:
My respect for emergency room physicians continues to grow. They are challenged with knowing something about almost everything in medicine. Unfortunately for them, their decisions are scrutinized, and they best not send someone home who needs to be treated or observed. Teenagers may need to go to the emergency room for many things: think appendicitis, a ruptured ovarian cyst, and an ectopic pregnancy. But emergency rooms are not the place to make the diagnosis of endometriosis.
The ill-prepared teenager who ends up in the emergency room because of an extremely painful menstrual period may end up having a nightmare experience. This experience often includes a pelvic exam, and ultrasound, blood work, and sometimes a CT scan all of which are normal. She is then told that there is nothing wrong, given pain medicine, and made to feel like a ‘baby.’ She may then be referred to a gynecologist. We can avoid this entire experience by evaluating the teenager’s complaints in the manner that I outlined above before she ends up in the ER. BUT don’t wait when symptoms are progressing, and never assume that because tests do not reveal anything this individual is simply a ‘wimp’!
STAY TUNED…
TREATING TEENAGERS TO FOLLOW IN PART B!
Disclaimer: any and all material(s) presented herein are offered for informational purposes only. Such material is not intended to offer or replace medical advice offered by your personal physicians or healthcare professionals. No information herein should be considered as party to any doctor/patient relationship. All contents herein are © copyright by Robert B. Albee, Jr., MD except where otherwise explicitly noted. All rights reserved. This material may not be reproduced or utilized in any form, including electronic or mechanical, photocopying, recording, or by any information storage and retrieval system except for personal or teaching use with prior permission. Thank you.

 Technically speaking, the surgical treatment of endometriosis rarely requires removal of the uterus (see prior article on ‘
Technically speaking, the surgical treatment of endometriosis rarely requires removal of the uterus (see prior article on ‘


 SUPPLEMENTS:
SUPPLEMENTS: HERBS:
HERBS: ACUPUNCTURE:
ACUPUNCTURE: HOMEOPATHY:
HOMEOPATHY: AROMATHERAPY:
AROMATHERAPY:
 HEAT/COLD APPLICATION: COLD!
HEAT/COLD APPLICATION: COLD! HEAT/COLD APPLICATION: HEAT!
HEAT/COLD APPLICATION: HEAT!